
Putting Out the Fire
New treatments bring relief in inflammatory muscle disease, but patience is required
 These days, you can find Giovanna Albers at home with her family in Imperial, Mo., or on the job as a hostess at LongHorn Steakhouse in nearby Sunset Hills, or swimming laps at the YMCA.
These days, you can find Giovanna Albers at home with her family in Imperial, Mo., or on the job as a hostess at LongHorn Steakhouse in nearby Sunset Hills, or swimming laps at the YMCA.
The trim, attractive, even athletic-looking 38-year-old radiates good health. So it comes as a surprise that her walk demonstrates profound weakness of her hip and thigh muscles, and that she occasionally falls.
Albers was only 19, newly married and "superactive" with karate, soccer and volleyball, as well as her job at a bank, when she began to notice that all was not well.
First, an injury to her upper left arm sustained during karate practice failed to heal, leaving a deep indentation in her deltoid muscle.
Then, early in 1985, shortly before her 20th birthday, Albers bent down to count the contents of her safe at the bank, and found she couldn't get up.
Myositis under the microscope
Albers was experiencing the first signs of what eventually would be diagnosed as polymyositis, which literally means "inflammation of many muscles," but which nowadays is defined as a misguided attack by the immune system on the body's muscles. It's one of many "autoimmune" or "self-immune" disorders, which occur when the body's tolerance for its own tissues mysteriously fails, allowing various organs to succumb to friendly fire that's normally reserved for bacteria, viruses and parasites.
Today, doctors recognize two other major types of myositis, or inflammatory muscle disease: dermatomyositis, in which the immune system attack results in damage to muscle, skin and sometimes other organs; and inclusion-body myositis, a disease of older adults in which inflammation plays a variable role and degeneration of muscles is a major factor. (For more on IBM, see "Advances in Inclusion-Body Myositis," April 2001; it won't be discussed here.)
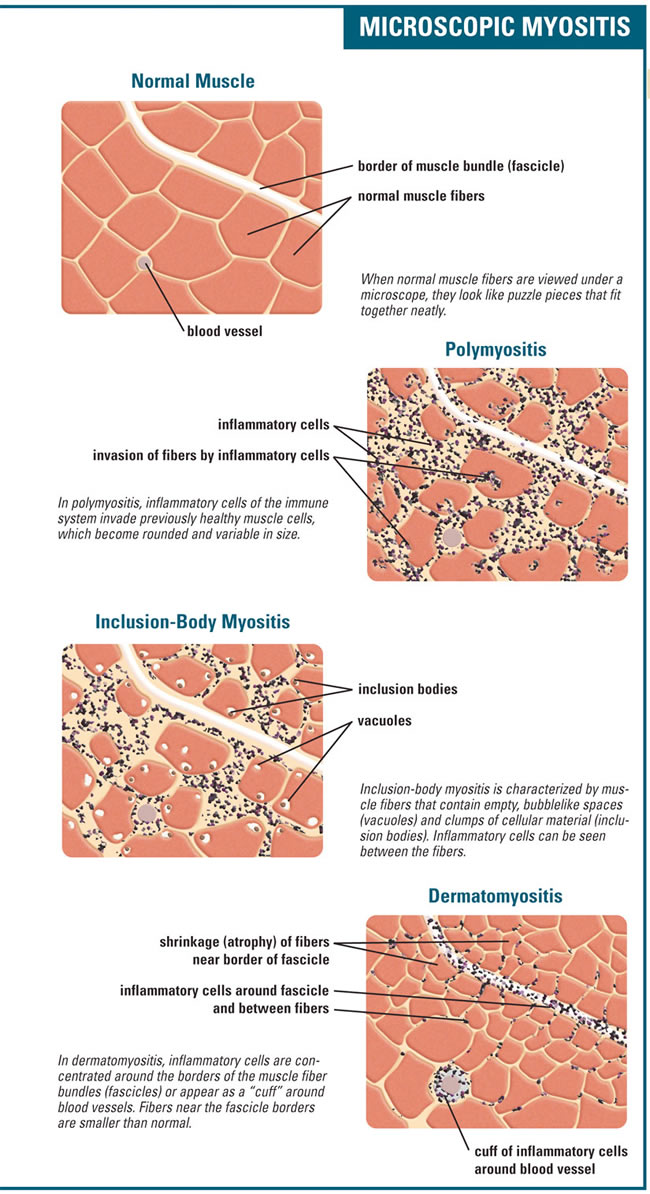
Experts make important distinctions among these diseases. (See graphic below.) Polymyositis seems to be a direct attack on muscle tissue itself, carried out mainly by the T-cells of the immune system. When experienced physicians read a muscle biopsy from a patient with PM, they see previously healthy muscle fibers being invaded by cells of the immune system (inflammatory "infiltrates"). They also see many dying and regenerating muscle fibers.
Dermatomyositis, literally "inflammation of the skin and muscle," was long considered simply "polymyositis with a rash." It's now known to have an entirely different underlying mechanism.
The primary target of the renegade immune system in DM appears to be the tiny blood vessels (capillaries) that supply muscle and skin, rather than these tissues themselves. The muscle biopsy sample, to the experienced eye, reveals loss of these capillaries, inflammatory infiltrates and many shrunken (atrophied) muscle fibers at the borders of muscle fiber bundles. (It's been thought that these border regions may have fewer capillaries to begin with and therefore suffer more from their depletion, leading to shrinkage of fibers.)
The attack in DM is largely carried out by the immune systems B-cells, the manufacturers of antibodies, also called immunoglobulins. These are proteins that act as the system's long-range artillery, sticking to cell membranes, such as those of the capillary walls, and causing their destruction.
More than muscles involved
Weakness -- almost always of the upper arms, hips or thighs, the "proximal" muscles for their nearness to the body's center -- is often the first sign of myositis but not always. And it may not be the first thing the patient, or even the physician, notices.
"I had no clue I was weak," says Jessica Aycock, a 23-year-old Tuscaloosa, Ala., woman who's recovering from a long bout with both DM and lupus. (Such combinations aren't uncommon between myositis and other autoimmune disorders, such as lupus or scleroderma.)
Aycock's first symptoms were persistent fevers and rashes that started during her pregnancy and refused to leave even after her baby, Jasmine, was born.
The myositis part of her disease wasn't recognized until formal strength testing revealed it.
Dermatomyositis in particular may make itself known with symptoms other than weakness, and this is especially common in children, says Lisa Rider, a pediatric rheumatologist (specialist in diseases of joints and related tissues) at the National Institutes of Health in Bethesda, Md.
Rider, who is studying myositis in children, is a senior clinical investigator at the NIH's National Institute of Environmental Health Sciences.
While DM is primarily a disease of skeletal muscles, she says, it also can be a systemic disease. "The patients are very tired," she notes, "and they can have swallowing trouble, changes in their voices [because of vocal cord abnormalities], arthritis [joint inflammation], and constipation or diarrhea."
Immunologic attack directed at the lungs or heart also can occur in DM, though less frequently in children than in adults. In many children Rider sees, the skeletal muscle in the chest wall is an immune system target. Weakness in this area can restrict lung expansion and lead to shortness of breath with exertion.
Children in particular, but also adults with DM, can develop what Rider believes may be inflammation of the fat just under the skin. This shows itself as small, tender bumps and is, in her view, likely to be a precursor of the large and uncomfortable calcium-containing deposits that often develop in this disease. Known as calcinosis and affecting about a third of children with DM, these deposits can be uncomfortable as well as causing self-consciousness in patients.
"The skin disease can be as debilitating as the muscle disease," Rider says of childhood DM. She and her colleagues are studying deposits after they've been surgically removed from patients to see how they form, what they contain and how to best treat them with medications.
Getting down to it
Diagnosing myositis isn't easy outside a major medical center where doctors have seen it before and know how to recognize it.
Marilyn Townsend of Mt. Morris, Mich., was in her late 60s and looking forward to an active retirement, when weakness in her thigh muscles began preventing her from going up or down stairs or getting into or out of her car.
She consulted three specialists, ending up with a diagnosis of late-onset limb-girdle muscular dystrophy. That misdiagnosis proved to be a stroke of luck, however, as it led her to the MDA clinic in East Lansing and a revised diagnosis of polymyositis.
Jessica Aycock kept running into doctors who would deal with one aspect of her increasing number of problems and then tell her that the others were "not my area," she says. "I went to all these doctors, and they couldn't diagnose me so they wouldn't treat me. They wouldn't get down to it."
Things weren't much easier for Albers either. After she had been mistakenly told she had the flu, hepatitis and lupus, and was so weak her husband and parents had to take turns helping her get through the day at home, her mother made a desperate call to Barnes Hospital in St. Louis and asked to see a specialist.
"She called, and they told us we couldn't have an appointment for six months," Albers remembers. She also remembers her mother's chilling next words: "In six months, my daughter will be dead." The appointment was moved up.
Albers originally saw rheumatologist Lewis Fischbein at Barnes, who diagnosed polymyositis and started her on treatment. Later, she attended the MDA clinic at the same center, now Barnes-Jewish Hospital at Washington University School of Medicine in St. Louis, under the direction of neurologist Alan Pestronk.
Permanent meds likely
It's often said that myositis is, if not a curable disease, at least a highly treatable one. Sustained recovery without continued medication does occur, as it did for Albers.
Neurologist Jonathan Goldstein, who directs the MDA clinic at Yale University School of Medicine in New Haven, Conn., and has a special interest in inflammatory muscle disorders, usually starts his myositis patients on high-dose corticosteroid (prednisone family) drugs and works toward getting them on low-dose steroids, although there may be many other treatments in between.
In his experience with adult myositis, cures are uncommon. He estimates that "greater than 90 percent" of his patients are unable to remain off medication entirely. "They can get down to 5 or 10 milligrams a day [of prednisone], but not completely off," he says.
In children, says Rider, the chances of cure are better. (Some 85 percent of the children with myositis that Rider sees have DM; about 8 percent have juvenile PM, a rare condition; and another 8 percent have rare forms of myositis or myositis mixed with another disease.)
"In children, the recovery is pretty good," she says. "About 30 percent recover fully, about another 30 percent recover for a period of time and then relapse, and the rest don't seem to recover," she says. As long-term follow-up studies are conducted, more fully recovered children are being discovered, she added.
Steroids for starters
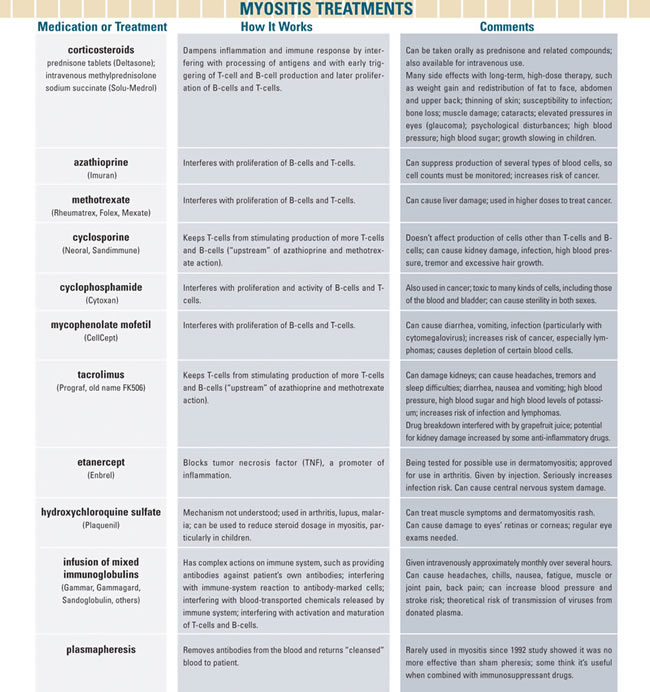
Treatments for myositis vary at different centers and among specialists, but almost all begin with corticosteroids, usually oral prednisone but sometimes intravenous methylprednisolone.
For best results, therapy should begin promptly and with high doses, most experts believe.
"It's important to get a diagnosis and start treatment early," says Andrew Engel, an MDA research grantee at the Mayo Clinic in Rochester, Minn., who sees myositis patients at the MDA clinic there, "because somehow the immune response reinforces itself. Responsiveness to therapy decreases as the interval between disease onset and the start of treatment increases."
Goldstein believes in starting with daily steroids like prednisone in a single, morning dose of 40 to 80 milligrams for adults, with doses based on weight in children, for two to three months -- "enough to make it work," as he phrases it.
"If you're going to get the side effects (See "Myositis Treatments" section below.), you might as well get the benefit," he says, noting that others may start with lower doses to avoid side effects but not bring the patient into remission. (There are alternative schedules for giving steroids, such as high-dose intravenous infusions every week or every other week.)
Beyond steroids
Goldstein, like many physicians, adds other drugs later, if they're needed to lower the prednisone dose or to mitigate steroid side effects, but there are some physicians who add a second drug from the start.
The medications most often added to prednisone or a related steroid are azathioprine (brand name Imuran) or methotrexate (Rheumatrex, others), both of which are potent and somewhat dangerous suppressors of the immune system but can help bring stubborn myositis under control with less dependence on prednisone. The latter can cause severe weight gain, high blood pressure, psychiatric changes, thinning of the skin, and loss of bone and muscle tissue if taken at high doses for more than a few weeks or months.
Goldstein notes that methotrexate is often the first choice of rheumatologists, while azathioprine is more often chosen by neurologists, a practice he attributes to differences in training.
Rider, for instance, prefers methotrexate to azathioprine, in part because it takes effect more quickly and in part, she says, because it seems to have more effect on the skin aspects of DM that are common in children.
She notes that many parents are reluctant to start a child on a drug that they view as dangerous chemotherapy. But in her experience, methotrexate is relatively safe and can spare the child from excessive steroid dosages for prolonged periods.
Later additions to the specialist's armamentarium against myositis may include still more potent and somewhat risky immunosuppressants, such as cyclosporine (Neoral, Sandimmune) and cyclophosphamide (Cytoxan), both of which are often used in cancer chemotherapy. (Methotrexate and azathioprine are used in certain cancers as well.)
These drugs kill rapidly dividing cells, such as those involved in an immune response. They're effective against tumors and autoimmune disease but often at the price of severely decreased infection resistance, loss of hair, gastrointestinal side effects, depletion of blood cells, and toxic effects on a growing fetus or even a nursing baby, depending on the exact drug, the dose and the duration of therapy.
New drugs
Several new drugs have entered the arena in recent years for other autoimmune diseases or for the control of unwanted immune responses against transplanted organs, and they're now being tried in myositis, with some success. As prices fall and experience increases, these medications are likely to play a larger role in myositis therapy.
Among these are etanercept (Enbrel), one of a new class of drugs that blocks the action of TNF, a substance secreted by certain immune system cells to augment the immune response.
Others are mycophenolate mofetil (CellCept), a potent and specific inhibitor of the proliferation of T- and B-cells, the main actors in the immune response; and tacrolimus (Prograf), which appears to keep T-cells from being activated.
The manufacturers of most of these drugs don't recommend taking them during pregnancy, or while breast-feeding.
Response to vaccinations, an important consideration in children, can be altered by these drugs, as well as by the disease itself. Reactions are unpredictable and can range from a vaccination that doesn't "take" because the immune system is too depressed by medication to respond to the vaccine; to augmenting the immune response the intention of vaccination and thereby causing a flare-up of the autoimmune disease; to, at least occasionally, causing the patient to contract the disease for which he or she is being vaccinated, if the vaccine contains a live virus.
 And, although it may seem paradoxical to add antibodies (immunoglobulins) to a system that seems to have more than its share of these proteins, the infusion of intravenous immunoglobulins has shown some success in myositis. They may be safer than some of the medications now used, especially in older people or those with complicating medical conditions that might make the use of potent immunosuppressants even more dangerous than usual.
And, although it may seem paradoxical to add antibodies (immunoglobulins) to a system that seems to have more than its share of these proteins, the infusion of intravenous immunoglobulins has shown some success in myositis. They may be safer than some of the medications now used, especially in older people or those with complicating medical conditions that might make the use of potent immunosuppressants even more dangerous than usual.
A procedure called plasmapheresis, in which antibodies are filtered out of the blood, was once thought to be helpful in myositis, but it's rarely tried today. A trial at NIH (in which Albers participated) found it to be no better than a placebo (accomplished by a "sham," or fake, pheresis). When results of the trial were published in the New England Journal of Medicine in 1992, some experts protested that pheresis must be used in conjunction with immunosuppressive medications, and this debate has never been settled with absolute certainty.
Trying the treatments
Giovanna Albers' weight soared from 140 to 200 pounds while she was on prednisone, which she describes as a humbling episode in her life. (She's since lost all the weight and has been able to resume her breakfasts of Snickers bars.)
"Not that I was such a vain person before," she says, "but it totally humbled me. It was such an experience for me to see how obese people get treated."
Albers was unable to try other immunosuppressants because she became pregnant shortly after she began her myositis treatment. She took prednisone during the pregnancy -- considered reasonably safe -- and her baby, Stephen, was born in good health though somewhat premature and temporarily stressed. Her pregnancy was considered high-risk, and she needed an emergency Caesarean section after the baby stopped moving two weeks before his due date.
The trial of plasmapheresis and a related procedure, leukapheresis (in which cells are removed), gave her nothing but "sore veins," she says.
She now takes a bone-building drug to offset the long-term prednisone effects but considers herself healthy, attractive, and more or less able-bodied again.
Jessica Aycock gained some 100 pounds on prednisone. At 5 feet 1 inch, she describes herself as a "little, short, fat person right now." She's slowly taking the weight off through a diet program and a mild exercise plan that involves walking in place.
 Fortunately, she's off prednisone now and has found CellCept to be her deliverance. "It worked perfectly" for both her DM and her lupus, she says, and as of the fall she was slowly being weaned from that drug as well.
Fortunately, she's off prednisone now and has found CellCept to be her deliverance. "It worked perfectly" for both her DM and her lupus, she says, and as of the fall she was slowly being weaned from that drug as well.
It's rare for prednisone not to help in myositis, side effects notwithstanding, but that was the case for Marilyn Townsend.
Fortunately, her physician helped her get approval through Medicare for treatment with intravenous immunoglobulins (IVIg), which she began in September 2002.
"After the first couple of months, it made a tremendous difference in my strength," she says, although she also experienced headaches and nausea at first until the rate of the infusion was slowed.
As of October, she was going to an infusion center in Flint three times a week for about five hours per treatment, during which she feels well enough to watch television, play cribbage, read or nap.
"IVIg has worked out really well," she says, although her doctor is now considering trying her on CellCept, which can be taken by mouth. "Dr. [David] Simpson is a good doctor," she says of her physician, who directs the MDA clinic in East Lansing. "He's caring and concerned and doesn't brush people off."
Rehab regimens differ
Medications are the mainstay of treatment in myositis, but physical therapy and exercise-based rehabilitation also have a crucial role, doctors say, even though they disagree on the details.
Lisa Rider says she sometimes has to restrain young patients from overdoing exercise, because she has found it can lead to flare-ups of the disease in damaged muscle tissue. "When kids feel tired or they feel muscle pain, it's time to stop," she says. "Some kids overdo it. They push too hard, and some of them flare after that."
Once their disease has stabilized, Rider prescribes a program of graduated rehabilitation, starting with range-of-motion exercises. Then the patient may progress to gentle muscle-strengthening exercises with a large elastic band, under the supervision of a physical therapist; and later move on to walking, cycling or swimming, the last of which is her preference. "It's good for joints and muscles," she says, "and it doesn't overstress the muscles."
Engel also favors swimming, as long as patients don't become tired or feel their muscles hurting. "Exercise should not be pushed," he says, "because it can worsen already damaged muscles."
Goldstein is a bit more enthusiastic about exercise, recommending swimming ("even in the worst off," he says), walking, bicycling or even running, depending on the person's capabilities. He draws the line, however, at lifting weights, saying this can damage muscle if there's inflammation present.
Specific triggers, specific treatments
Research goals now being pursued in myositis include: drugs that act specifically on one part of the immune system; identification of the particular protein targets antigens that set off the immune response to muscle or capillaries; environmental and genetic factors that cause the immune system to turn on the body's own tissues; and more understanding of the subtypes within each general myositis group. (For updates on clinical trials, watch this publication, and check www.clinicaltrials.gov.)
Identifying antigens is important because, "If you knock out all the T-cells, you remove useful T-cells, so you have to be careful," Engel notes. "If you found a specific peptide [protein part] that was acting as an antigen, then you could try to desensitize the immune system to that peptide or inhibit the receptor that can see that peptide."
Albers' physician in St. Louis, Alan Pestronk, says the careful identification of different types of PM, DM or IBM patients would go a long way toward individualizing treatment and minimizing side effects and therapy delays. For example, he makes a distinction between PM with and without abnormalities in the mitochondria (the cells energy-producing units), a difference that can be seen on a muscle biopsy if it's carefully sought. The type with mitochondrial involvement affects mostly older adults, such as Marilyn Townsend, and generally responds poorly to corticosteroids.
Lisa Rider's research group is studying myositis-associated antibodies, some of which have been noted in patients with other autoimmune diseases.
She and her colleagues at NIH and elsewhere are also studying methods to make myositis clinical trials more accurate, by developing clear measures of improvement or lack of it in a fluctuating disease; investigating genetic and environmental risk factors for myositis; and analyzing the formation of calcium deposits. She's also a co-investigator on a trial of infliximab (Remicade), a TNF blocker.
"Immune-mediated diseases in general are all being worked on," Goldstein says. "There's supposed to be a tolerance to self-antigens, and breakdown of tolerance is not well understood, though it's the subject of much research." More specific immunosuppression -- "shutting off the cells that are attacking the target but not all immune system cells" -- would be ideal, he says.
Wiser and emotionally stronger
"All of this happened because of the pregnancy [the hormonal changes of pregnancy can trigger an autoimmune disease], but that's also the best thing that ever happened," says Jessica Aycock. "Jasmine is great."
Giovanna Albers is now back to her normal weight of 130 pounds, slim for her 5-feet-6-inch frame and is trying to eat more healthfully. She says she's no longer an "exercise buff" but that she loves swimming because she's not working against gravity.
"I live and breathe in the water," she says. "It makes me feel normal."
She also loves her job at LongHorn Steakhouse, where she has been a hostess for about six years. She can no longer bus tables and there are days when even hostessing can be a problem. At those times, she says, her supervisors give her office work to do.
"There's been no discrimination there at all — not any because of my Puerto Rican background and not any from my disability," she says of LongHorn.
Another thing Albers loves is sunlight, and she believes it helps any residual PM she has.
(By contrast, excess sun exposure can be a real hazard in dermatomyositis. Lisa Rider instructs her patients to wear sunscreen and protective clothing, and sometimes even asks children to stay indoors during the peak sun hours.)
"I feel so much better in the spring, summer and fall," says Albers, not only because of the sunlight-poor colder months but because of the weight of heavier clothing during the winter.
"But," she says, "I just do what I can. A lot of health is mental anyway."
When asked to tell her story for Quest, Albers commented, "If it helps one other person go through what I have already gone through and come out of it a lot wiser and stronger emotionally, well then, just maybe there was a purpose for it all."
MDA Resource Center: We’re Here For You
Our trained specialists are here to provide one-on-one support for every part of your journey. Send a message below or call us at 1-833-ASK-MDA1 (1-833-275-6321). If you live outside the U.S., we may be able to connect you to muscular dystrophy groups in your area, but MDA programs are only available in the U.S.
Request Information
