
When Form Meets Function: Exploring Surgery to Restore Muscle Power in FSH Dystrophy

The trouble started for Claire Walker when she was in kindergarten, when her physical education teacher noticed that she couldn't do sit-ups like the other children and that her back seemed "lopsided." Claire's parents took her from their home in Louisiana to see Yadollah Harati, an MDA-affiliated neuromuscular disease specialist at Baylor College of Medicine in Houston.
There, she learned she had facioscapulohumeral (FSH) muscular dystrophy, a muscle-wasting disease that mostly affects the muscles of the face and upper body but can also affect the back and legs.
Claire had spine-straightening surgery at age 9, which solved her back problems, but later, she began having problems using her arms. Each of her shoulder blades (the medical term is scapulae) "would flip out like a wing" when she tried to reach for things, and that part of her body was a constant sore spot. By the time she was in college, "just picking up a glass of water got to be a little bit difficult. I would drink more to the side, not right out in front of me. It got old."
Barbara Williams has similar childhood memories. In school in Oregon, she couldn't raise her hand in class without supporting it with the other arm. "The nuns would scream at me," she says.
In her 20s, Williams worked as a grocery cashier but was getting weaker. Having to stand up all day wasn't the hard part, she recalls. "It was the reaching out to grab things to scan them. I was achy around my shoulder blades all the time." Williams, who is left-handed, says her right shoulder always gave her more trouble than her left.
Williams had known for some time that she and her brother had FSH dystrophy and had seen doctors in the Portland area. She'd tried massage therapy and other pain-relieving techniques that didn't seem to be helping much. In the mid-1980s, she consulted a surgeon, who advised against an operation, telling her she'd lose so much mobility from such surgery that she'd never be able to brush her teeth or take care of her hygiene needs. She accepted this verdict.
A 'marvelous operation' — for some
Irwin Siegel, an orthopedic surgeon who co-directs the MDA clinic at Rush-Presbyterian-St. Luke's Medical Center in Chicago, is a pioneer in the field of thoracoscapular fusion surgery. This operation attaches the shoulder blade (scapula) to the back of the rib cage (thorax) and can be helpful for the problem affecting Walker, Williams and others with FSH dystrophy.
Occasionally, the operation may be useful in other neuromuscular disorders, such as limb-girdle or Becker muscular dystrophies, but in the great majority of these cases, upper body weakness is more generalized than it is in FSH dystrophy, which renders the procedure useless.
Unfortunately, Siegel says, thoracoscapular fusion ("scapular" fusion for short) is "rarely performed, even today, because relatively few patients or doctors are aware of its existence."
Siegel calls the surgery a "marvelous operation," but cautions that it has to be done by the right surgeon on the right patient.
The right surgeon, he notes, is experienced with shoulders and with muscular dystrophy, and the right patient is one with weak scapula-stabilizing muscles but a strong deltoid — the muscle that connects the upper arm bone (humerus) to the shoulder blade and collar bone.
In FSH dystrophy, Siegel explains, the muscles that normally hold the shoulder blade in place are usually so weakened by young adulthood that the arm-lifting deltoid loses its mechanical advantage. When the scapula doesn't provide a stable platform for the deltoid to pull against — a condition called scapular winging, because the scapula sticks out like a wing when the person tries to lift his arm — even a relatively strong deltoid can't raise the arm very high or for very long.
One of the most troublesome deficits occurs when the person tries to move his arm up high in front of the body (called flexion), the type of movement needed in reaching for a glass in a high cupboard or a book on a high shelf. Equally problematic is reaching out to the side (a movement called abduction), such as when pulling grocery items from a conveyor belt. These movements are especially difficult if they have to be sustained or repeated.
 With help from Harati, their physician in Houston, Walker's parents found orthopedic surgeon J. David Thompson, who practices at Cardinal Glennon Children's Hospital in St. Louis.
With help from Harati, their physician in Houston, Walker's parents found orthopedic surgeon J. David Thompson, who practices at Cardinal Glennon Children's Hospital in St. Louis.
Thompson, who says Siegel was "instrumental in my getting started [in scapular surgery] and generous with his time," has now performed more than 40 scapular fusions, mostly in people with FSHD. He agrees with his mentor that in the right hands and with the right patient the operation can be very helpful in improving function.
Fortunately, Thompson says, there's a fairly easy and accurate way to tell who will benefit from the surgery. Known as the manual compression test, it involves having an examiner hold the scapula flat against the back, simulating temporarily what the surgery would do permanently, while the patient tries to lift his or her arm up and out.
If he can suddenly lift the arm higher and for longer with the examiner's hand pressed to his back, the patient's deltoid is likely to be strong enough to gain considerable benefit from scapular fusion surgery.
The manual compression test can be dramatic. "That's when they all decide they want the operation," Siegel says, noting that patients are often mazed at how strong their upper arm muscles are once the shoulder blade is held steady.
Not for the casual surgeon
"It's helped out tremendously," Walker says of the surgery she had on one shoulder when she was 20 and the other at 21. (Her surgeon, Thompson, says most of his patients have been in their late teens or 20s, with a few in their 30s.)
Thompson is enthusiastic, too, but, he cautions, scapular fusion is a "major operation." Significant postoperative pain and a prolonged period of restricted arm movement are certain, while respiratory and other complications aren't uncommon.
Thompson advises people to have one shoulder operated on at a time, so they'll have at least one arm free for activities of daily living during the healing process.
Siegel recommends finding someone who has experience with thoracoscapular fusion.
"It's not something for the casual surgeon," he cautions. "It's not a common operation even for someone who specializes in shoulder surgery."
Procedures vary
The actual procedures used to attach the scapula to the ribs and the types of postoperative restrictions that follow vary somewhat among doctors and even for patients who have the same doctor. "There isn't a lot of cookbook about neuromuscular disorders," Thompson says.
In the past, methods of pinning down the scapula ranged from the very flexible, such as synthetic mesh materials or fascia (fibrous tissue), to the very firm, using metal screws.
Neither method is as popular today. The flexible attachments, while effective at first, stretched out over time and failed to hold the shoulder blade down. Screws, Siegel says, have a good chance of protruding through the bone and damaging or irritating soft tissue in the chest area.
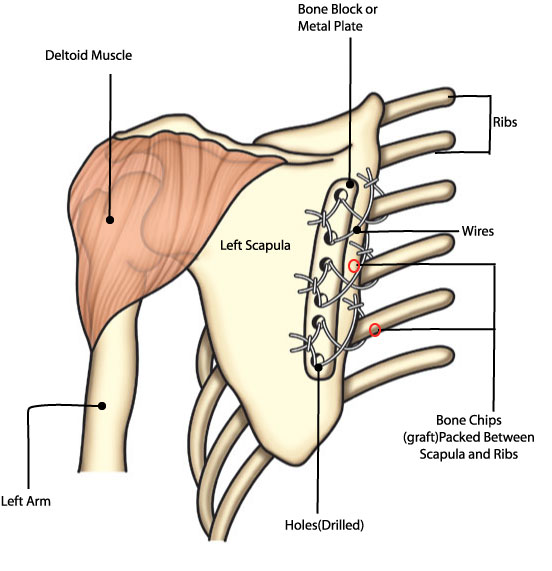
Today, surgeons are likely to use flexible wires combined with a bone graft (small pieces of bone, taken from the patient or from another source) to do the attachments. Holes are drilled through the scapula and wire is wound around three to five ribs.
Siegel reinforces the attachment with a metal plate over the scapula, through which holes are also drilled, matching those in the bone underneath. (Think of the plastic strip that often reinforces the margin of loose-leaf notebook dividers to keep the rings from tearing the paper with wear.)
Thompson prefers to use blocks of bone to substitute for the metal plate and says experiments have convinced him that a special way of threading and tying the wires called a "tension band wiring technique" provides a durable but flexible connection. (See illustration above.)
Wires may break some time after surgery, but that normally doesn't matter once the bone graft has sealed the attachment. In fact, if the wires become uncomfortable, they can be removed later.
Surgeons know that taking a bone graft from the patient — most often from the hip — exposes him or her to a separate procedure, with more pain and a second incision and scar. But, at least for some, it's still a better way to go than using donated bone, which is available from bone banks. Thompson calls the patient's own bone the "gold standard" for grafts.
Postoperative routines vary, too.
Siegel's patients stay in a soft arm immobilizer for about three weeks (see below) and then use a sling for a while longer. At about six weeks, his patients start exercising with the arm supported by another person and then, at 10 to 12 weeks, they exercise more vigorously to keep the deltoid muscle strong.
Thompson's regimen involves arm immobilization for about eight weeks after surgery, followed by physical therapy.
His patients are instructed to stay away from vigorous activities for six months. He also advises them to stay out of school for six weeks or an office job for three to six weeks.
Getting over it
Both of Walker's surgeries went pretty smoothly, she says, especially the second one, but there were some rough periods.
 She was in the hospital for 10 days with the first procedure and a few days less with the second. After each surgery, she had excess fluid buildup and irritation of the membrane around her lung, with pain requiring extra medication.
She was in the hospital for 10 days with the first procedure and a few days less with the second. After each surgery, she had excess fluid buildup and irritation of the membrane around her lung, with pain requiring extra medication.
The prolonged post-op immobility wasn't easy, either.
"You have to keep your arm to your side from the elbow up for eight weeks," she says. "There's a bone graft in between the ribs and the shoulder blade with wire keeping it together that can only take so much pressure, so you're restricted in what you can lift up to the point where the bone graft has solidified."
Thompson instructed Walker not to lift heavy things for nine months. She did physical therapy for two months after each surgery, and she still does some muscle-toning exercises on her own.
Now 22 and working in the sales department of a company that markets outdoor equipment shelters, Walker has had no regrets about the surgery. She says her posture and appearance are much better, and her function has greatly improved.
"My back is flat around my shoulders, which is nice," Walker says, "and I think I gained probably 60 or 70 degrees of flexion."
Williams, now 42 and living just outside Portland in Clackamas, Ore., is happy about the surgery she had many years after the first doctor turned her down. She wishes she hadn't waited so long.
"I think I lost an awful lot of muscle," she says of the years between the first and second surgical consultations. "I think I would have been stronger and recovered faster when I was young, and that I would have gotten more movement out of [the operation] if I had been younger and hadn't lost so much muscle to start with."
Williams eventually left the grocery store, went into office work and then stopped working entirely to stay home with her two children. She had scapular fusion surgery on her right shoulder shortly before turning 40 in 2001. Her doctor was Kevin Smith of the University of Washington Medical Center in Seattle.
She used donated bone rather than undergo the procedure necessary to use her own bone, and she wore only a sling for about six weeks after surgery. Her doctor had her doing mild exercises the second day after her operation, using a pulley system hooked to the door.
Williams says she's lost some ability to reach to the side, such as when passing things at the table or reaching across the front seat of a car, but she's able to reach up higher and lift better. She can now grab a gallon of milk from the refrigerator and put it on the counter "like anyone else," while before the surgery, the container would just "flop down by my side."
Best of all, she says, "I don't have that horrible burning pain between the shoulder blades and along the spine anymore."
Smith was also the surgeon for Jesse McKee, an 18-year-old who works in his grandfather's hardware and construction business in rural Whitehorn, Calif. McKee had each of his scapulae fused when he was 16, in separate procedures about six months apart. He made a rapid recovery each time, a fact that he and his mother, Maryellen, attribute partly to his youth and general fitness.
McKee also used donated bone rather than his own. He used a sling for about six weeks and then gradually began lifting things, progressing from coffee cups to 5-pound weights and eventually to the 40-pound bags of soil he's now able to throw into the back of a truck. He didn't do any special exercises or therapy.
He says he's definitely stronger and looks better (he used to be teased at the swimming pool about being "slouched over"), but he's not quite as flexible as he was before the surgery. Recently, he's also developed some problems with the thumb and a finger on his left hand, which he suspects may be from a stretched or pinched nerve, a problem he plans to ask his surgeon about soon.
A significant chunk of life
The expected drawbacks of scapular fusion surgery include postoperative pain, with morphine usually needed for several days; weeks to months of relative immobility on the operated side, with possible loss of muscle power, at least in the short run; and exposure to general anesthesia in a fairly lengthy surgery. (FSHD isn't particularly likely to cause problems related to anesthesia, but the surgical team should be aware of the patient's muscular dystrophy. See "Coping with Anesthesia," Quest, June 2000.)
There's a fairly large scar from the incision over the scapula, although appearance may be improved through better posture and a flatter back; and there can be some loss of flexibility because of the pinning of the scapula to the rib cage.
Scapular fusion operations are expensive (although insurance companies don't seem to have a problem in covering them for FSHD patients), and they usually require at least several weeks of time away from work with potential loss of income.
Thompson says the surgery "takes a significant chunk out of a person's life. By the time you do both sides, you've taken out a year." Therefore, he says, people "need to be committed to doing it and understand what they're getting into to get the best result."
Risks that are unexpected but deserve consideration include enough blood loss to require transfusions; fracture of the ribs or scapula during surgery; failure or breakage of the attachment of the scapula to the ribs; puncture of one of the membranes surrounding the lungs, with air or blood entering the chest cavity and compressing a lung (a problem that can usually be easily treated); irritation of one of these membranes with excess fluid production and pain (pleurisy or pleural effusion); infections; and damage, usually temporary, to the nerves that control the arm.
Because the scapular fixation reduces rib movement a little bit, there can be a small decrease in the degree to which the lung can expand on the operated side. Usually, in people with FSHD, this slight loss of lung capacity isn't important, studies show.
Siegel says the operation requires three or four hours in the operating room and can be arduous for the surgeon as well as the patient. He doesn't perform such long procedures himself anymore, although he's taught many younger specialists, including some overseas.
A good result
Siegel points out that techniques and approaches to rehab have improved while he's been in practice and will continue to do so.
 "Over the years we've used less and less restrictive immobilization," he says. "We got rid of the plaster cast and went strictly to the soft arm immobilizer, and we gradually have begun to use that for less and less time. The techniques have improved, and the materials have improved," he notes, and so has the understanding of how surgery and muscular dystrophy interact.
"Over the years we've used less and less restrictive immobilization," he says. "We got rid of the plaster cast and went strictly to the soft arm immobilizer, and we gradually have begun to use that for less and less time. The techniques have improved, and the materials have improved," he notes, and so has the understanding of how surgery and muscular dystrophy interact.
"When you take a person with muscle disease and hold them immobile, they atrophy rather profoundly," he says, and this atrophy (shrinkage) of muscles can be hard to reverse later. "We may have been unduly cautious," he says of the overly restrictive post-op regimens of the past. "But that's the learning curve."
Thompson says the secret to success, from the surgeon's point of view, is to "take a good history, do a good exam, identify patients who are good candidates for surgery, and be meticulous about the technique and the aftercare."
But, he cautions, "this is not an operation where the doctor does something and you're fine. The doctor does something and you [the patient] are going to make it work. The patient has to undergo a period of rehabilitation to make it work well.
"The motivated patient is really the key to a good result."
Both sides now?
Although a few people have undertaken scapular fusion surgery on both shoulders during the same operation, orthopedic specialist J. David Thompson says he's only done it once, more than 10 years ago, and advises against it.
The patient, a nurse in her 30s with FSHD, had arranged for relatives to take care of her children and thought she could keep both arms immobile for the required amount of time. But, Thompson says, that proved impractical, and one side, because of use by the patient, failed to fuse.
A second operation was necessary, and that, unfortunately, resulted in some nerve damage that took seven months to resolve.
"I'll never do it again," he says of the two-sided procedure. "She was very careful, but the patient cannot protect [both shoulders] enough. I think it was my mistake to do both at the same time."
Leslie Van Alstyne couldn't agree more. Now 25 and a medical equipment evaluator in the Philadelphia area, Van Alstyne has just about recovered from extensive surgery for her FSHD-related problems over Christmas break during her sophomore year in college.
The surgeon, a specialist at a prestigious Boston medical center who was recommended by one of Van Alstyne's doctors in Pennsylvania, suggested that he could operate on her spine and both scapulae at the same time and have her back in school by late January. That, however, wasn't what happened.
Van Alstyne says she now realizes that the surgeon wasn't very familiar with FSH dystrophy and didn't recognize how much leg weakness she had — and that it would worsen, at least temporarily, from lack of muscle use after surgery. Completely immobilized from the three procedures, Van Alstyne was in great pain and unable to do anything for herself for months.
She thinks that nurses who were trying to move her may have inadvertently broken one of the scapular fusions when they were lifting her in a blanket "like a log" shortly after surgery. In any case, one side failed to heal and had to be fused again later.
Meanwhile, Van Alstyne missed an entire semester of college, graduated late, and had to work for some time to regain her physical and psychological confidence.
In hindsight, she says, she would have made sure the doctor understood more about her muscular dystrophy. But she's glad she had the fusion surgeries.
"Cosmetically, it was a great thing," she says, and she's gained some range of motion and the ability to lift her arms higher. She does water therapy and walking to maintain her strength and is able to work on a computer all day and travel as necessary for her job.
She says she'd do it all again — but one side at a time.
MDA Resource Center: We’re Here For You
Our trained specialists are here to provide one-on-one support for every part of your journey. Send a message below or call us at 1-833-ASK-MDA1 (1-833-275-6321). If you live outside the U.S., we may be able to connect you to muscular dystrophy groups in your area, but MDA programs are only available in the U.S.
Request Information
